
At clinicals, you cannot think about every single step in careful detail and do your job as a nurse at the same time. You collect your patient's vitals, look at their chart, listen to them, and suddenly you are expected to combine this data and make a logical nursing care plan. This is where many nursing students lose the most time. When that happens, nursing care plans (NCPs) provide you with a structured guide to link patient data together, connect it with a nursing diagnosis, and then create an action plan that you can implement for your patient.
To assist you with understanding the ADPIE framework, I brought together 10 free nursing care plan examples so you can see how to build one yourself.

Exhausted From Clinicals?
Deadlines aren’t going anywhere. Let professionals handle the writing so you can stay rested.
Nursing Care Plan Examples for Students
Before we get to the nursing care plans examples, let's precisely describe what we are looking at. A nursing care plan is a sequence of decisions. It starts with patient data collection, then that assessment helps you shape the nursing diagnosis so you can find the right interventions. A strong nursing care plan sample makes that structure easily visible. You can trace each step and see that the logic holds from start to finish.
Nursing Care Plan Example #1: Acute Pain
Topic: Postoperative Abdominal Surgery Pain
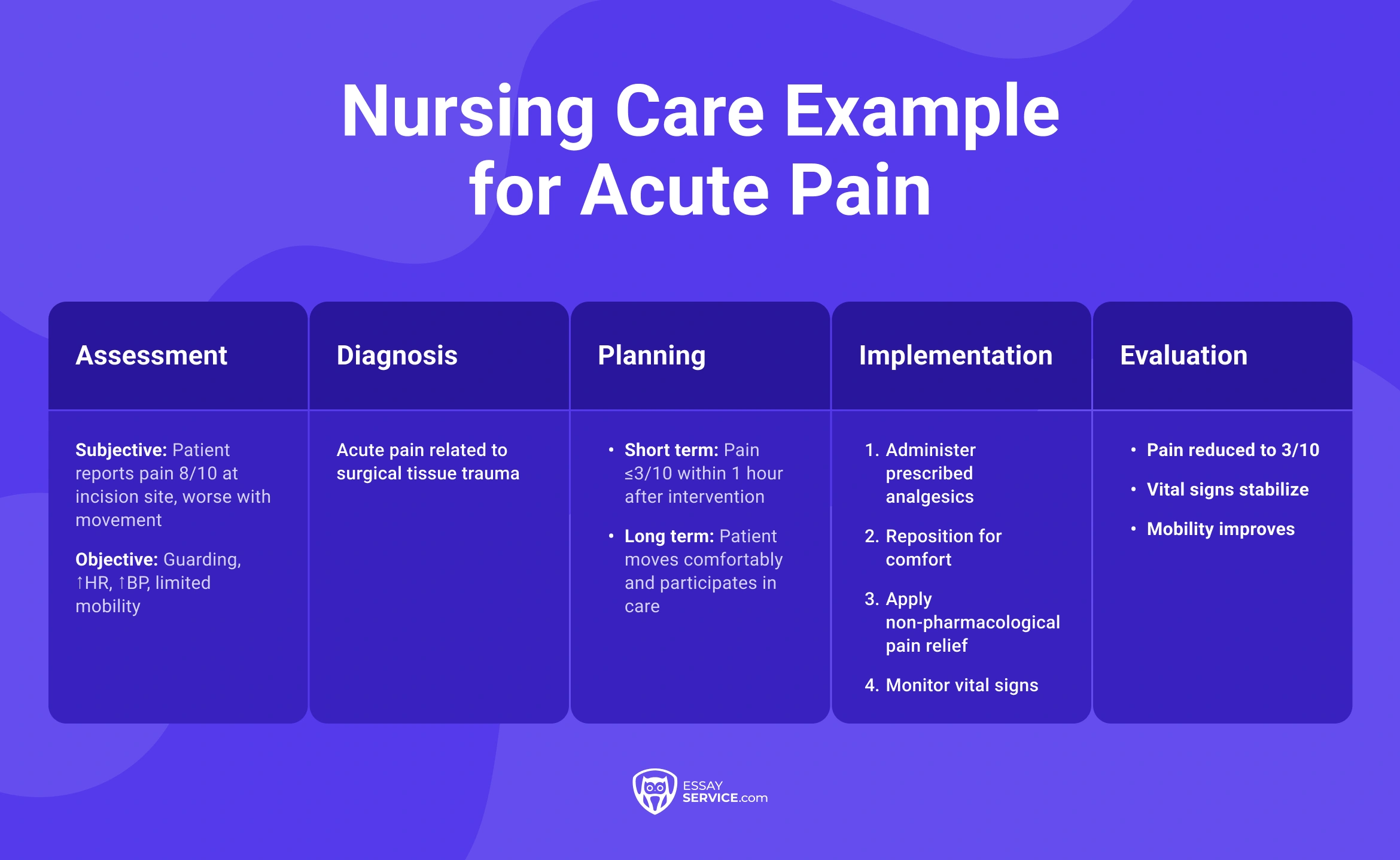
- Assessment: Patient reports pain level 8/10 at incision site; guarding behavior noted; elevated blood pressure; increased heart rate; limited mobility; facial grimacing
- Diagnosis: Acute pain related to tissue trauma secondary to surgery
- Planning: Patient will report pain reduced to 3/10 within 1 hour after intervention; patient will demonstrate improved comfort and ability to move
- Implementation: Administer prescribed analgesics; reposition patient for comfort; apply non-pharmacological pain relief techniques; monitor vital signs; educate patient on pain management strategies
- Evaluation: Patient reports pain reduced to 3/10; vital signs stabilize; patient shows improved mobility and comfort
Nursing Care Plan Example #2: Hypertension
Topic: Uncontrolled Hypertension with Medication Nonadherence
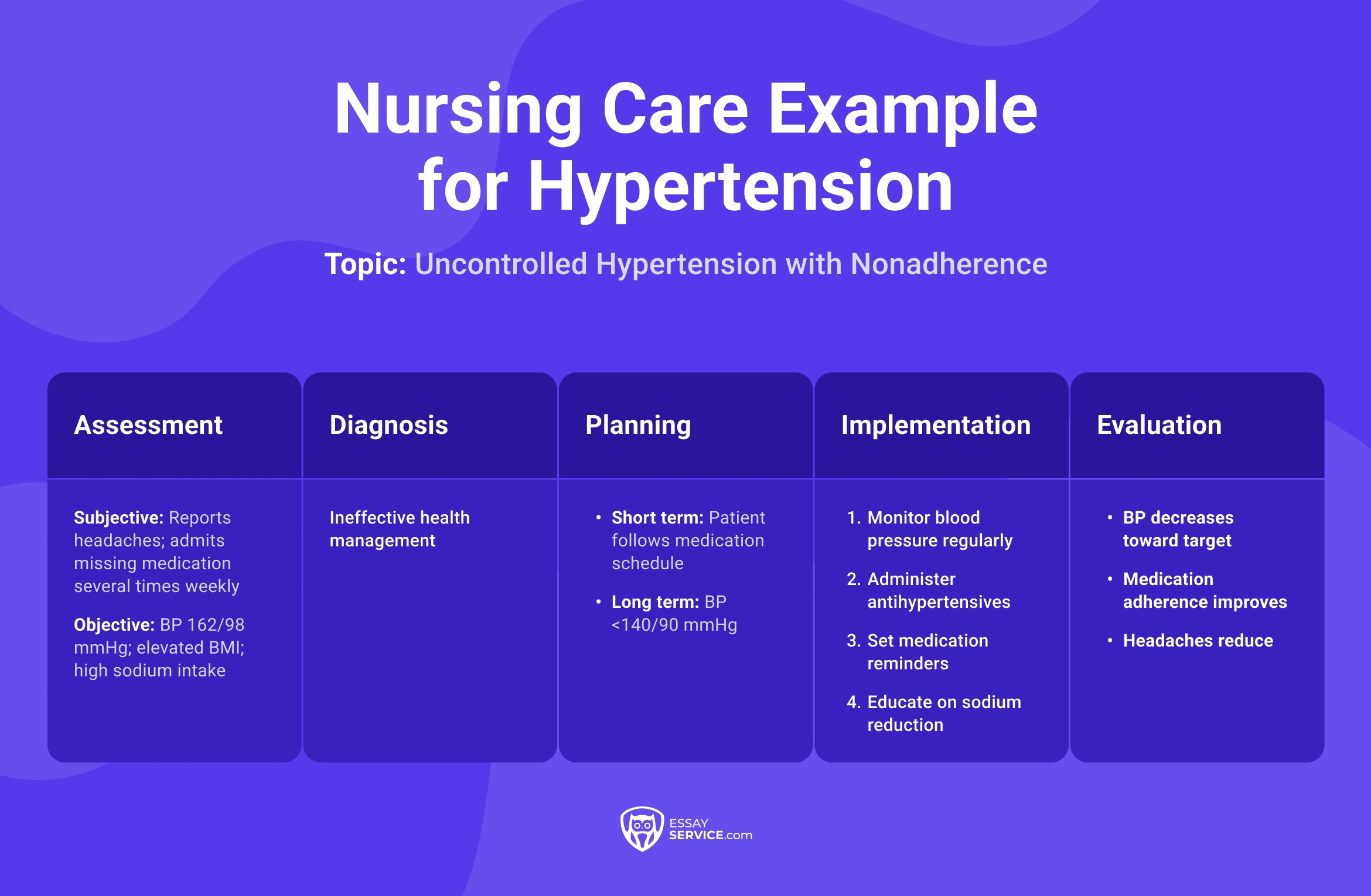
- Assessment: Blood pressure 162/98 mmHg on two readings 10 minutes apart; patient reports morning headaches; admits missing medication 3–4 times per week; sodium intake high based on 24-hour recall; BMI elevated; medical history includes chronic hypertension
- Diagnosis: Ineffective health management related to inconsistent medication use and high sodium intake
- Planning: Blood pressure reduced below 140/90 mmHg within two weeks; patient correctly states medication schedule; patient identifies two high-sodium foods to limit; patient reports consistent daily medication use
- Implementation: Check blood pressure every shift; administer antihypertensives as prescribed; set phone reminder with patient for medication timing; provide quick label-reading guidance for sodium content; document adherence in daily log; notify healthcare providers if readings stay above 150/90 mmHg
- Evaluation: Blood pressure decreases to 148/92 mmHg within several days; patient follows medication schedule without missed doses; patient avoids identified high-sodium foods; headache frequency reduced
Nursing Care Plan Example #3: Diabetes
Topic: Type 2 Diabetes Mellitus with Poor Glycemic Control

- Assessment: Fasting blood glucose 198 mg/dL; postprandial glucose above 250 mg/dL; HbA1c 9.2%; patient reports frequent urination, increased thirst, and fatigue; inconsistent use of prescribed insulin; dietary intake high in refined carbohydrates; patient unsure how to adjust insulin based on meals
- Diagnosis: Unstable blood glucose levels related to inconsistent insulin use and inadequate understanding of glucose management
- Planning: Blood glucose maintained within target range (fasting 80–130 mg/dL); patient demonstrates correct insulin administration technique; patient explains timing of insulin with meals; patient identifies two dietary adjustments to reduce glucose spikes
- Implementation: Monitor blood glucose before meals and at bedtime; administer insulin per sliding scale; demonstrate proper injection technique and site rotation; provide focused teaching on carbohydrate intake and meal timing; assist patient in creating a simple daily glucose log; reinforce recognition of hyperglycemia symptoms; coordinate with healthcare providers if glucose remains above 180 mg/dL
- Evaluation: Blood glucose trends decrease toward the target range; patient performs insulin administration correctly; patient maintains glucose log with consistent entries; symptoms such as excessive thirst and fatigue improve
Nursing Care Plan Example #4: Pneumonia
Topic: Community-Acquired Pneumonia with Impaired Gas Exchange
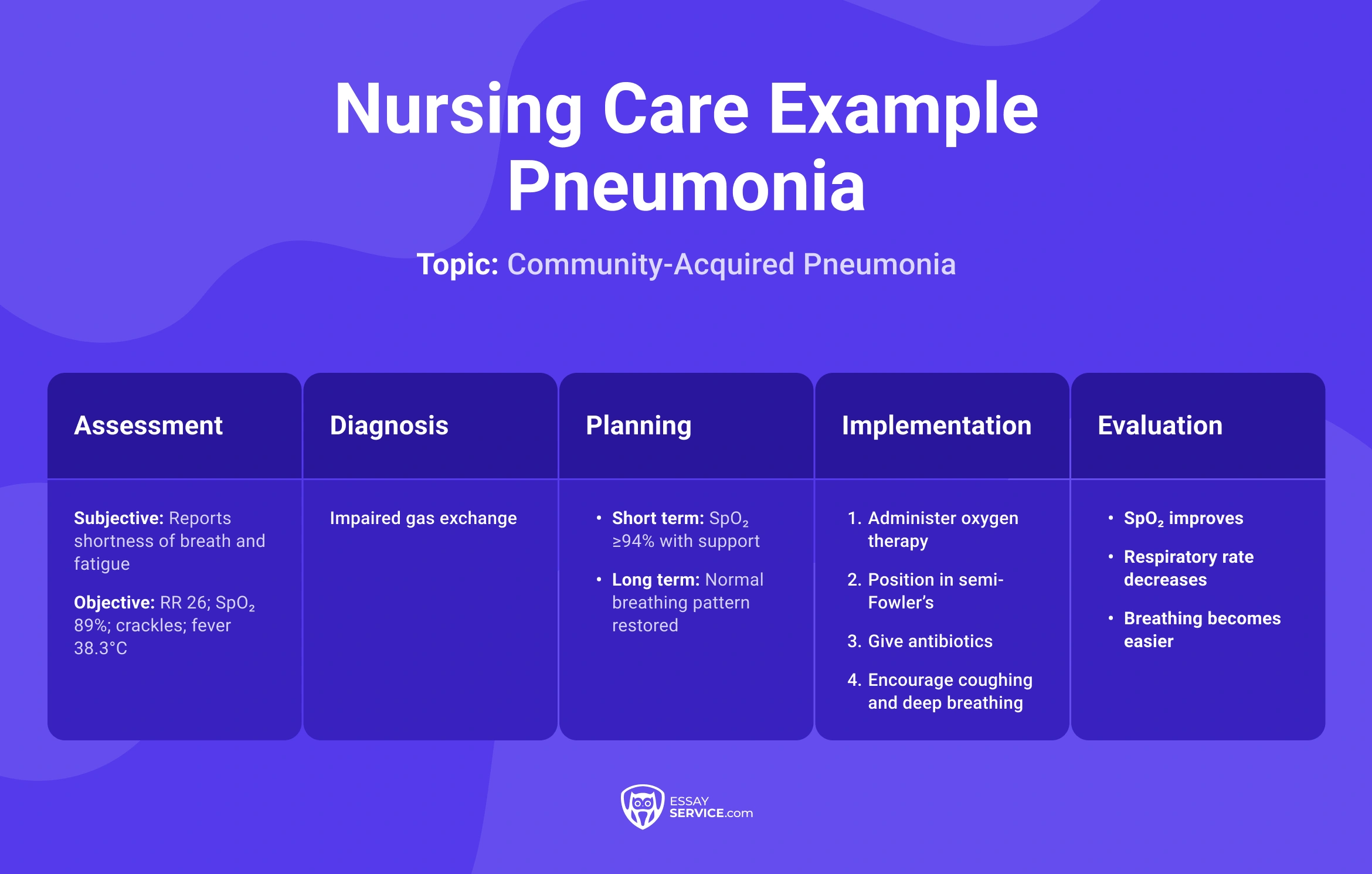
- Assessment: Respiratory rate 26/min; oxygen saturation 89% on room air; crackles auscultated in lower lobes; productive cough with yellow sputum; temperature 38.3°C; patient reports shortness of breath on minimal exertion; chest X-ray confirms consolidation
- Diagnosis: Impaired gas exchange related to alveolar inflammation and fluid accumulation
- Planning: Oxygen saturation maintained above 94% with support; respiratory rate reduced below 20/min; patient demonstrates easier breathing at rest; sputum production decreases and becomes clearer
- Implementation: Administer oxygen via nasal cannula at 2–4 L/min as prescribed; monitor oxygen saturation every 2–4 hours; position patient in semi-Fowler’s position; encourage deep breathing and coughing every 2 hours; administer prescribed antibiotics and antipyretics; monitor temperature and lung sounds; ensure adequate fluid intake to help thin secretions; collaborate with healthcare providers if oxygen needs increase
- Evaluation: Oxygen saturation improves to 94–96%; respiratory rate decreases; breath sounds show reduced crackles; sputum becomes less thick; patient reports decreased shortness of breath
Nursing Care Plan Example #5: Infection
Topic: Surgical Site Infection with Delayed Wound Healing

- Assessment: Temperature 38.1°C; incision site red and warm; purulent drainage present; localized swelling; patient reports increasing pain at wound site (6/10); WBC count elevated; dressing saturated within 8 hours; medical history includes recent abdominal surgery
- Diagnosis: Infection related to bacterial invasion at the surgical site
- Planning: Patient will show reduced signs of infection within 72 hours; wound drainage decreases; temperature returns below 37.5°C; patient reports pain reduced to 3/10; wound begins to show signs of healing
- Implementation: Monitor temperature every 4 hours; assess wound appearance and drainage each shift; perform sterile dressing changes as ordered; administer prescribed antibiotics on schedule; maintain strict hand hygiene; educate patient on avoiding contamination; document wound size, color, and drainage; notify healthcare providers if drainage increases or fever persists
- Evaluation: Temperature stabilizes within normal range; drainage decreases and becomes less purulent; redness and swelling reduce; patient reports lower pain level; wound shows early healing signs
If you've mastered the nursing care plan creation already and need to handle other medical assignments, reach out to a writer from our professional nursing essay writing service.
Nursing Care Plan Example #6: Congestive Heart Failure
Topic: Fluid Volume Overload in a Patient with Chronic Heart Failure

- Assessment: Blood pressure 148/92 mmHg; heart rate 104 bpm; bilateral lower extremity edema (2+); weight gain of 2.5 kg over 3 days; shortness of breath on minimal exertion; crackles in lung bases; oxygen saturation 92% on room air; patient reports difficulty lying flat
- Diagnosis: Excess fluid volume related to impaired cardiac function
- Planning: Patient will show reduced fluid retention within 72 hours; weight decreases by at least 1 kg; edema reduced; oxygen saturation maintained above 94%; patient reports improved breathing
- Implementation: Monitor daily weight at the same time each morning; assess edema and lung sounds every shift; administer prescribed diuretics; track intake and output accurately; position patient in high-Fowler’s position; limit fluid intake as ordered; educate patient on low-sodium diet; notify healthcare providers if weight increases more than 1 kg in 24 hours
- Evaluation: Weight decreases gradually; edema improves; lung sounds show fewer crackles; oxygen saturation stabilizes; patient reports less shortness of breath
Nursing Care Plan Example #7: Stroke
Topic: Acute Ischemic Stroke with Impaired Mobility and Swallowing Risk

- Assessment: Sudden onset right-sided weakness; facial droop observed; slurred speech; blood pressure 170/96 mmHg; difficulty swallowing noted during initial screening; decreased grip strength on affected side; patient unable to maintain balance when sitting unsupported; CT scan confirms ischemic stroke
- Diagnosis: Impaired physical mobility related to neuromuscular impairment; risk for aspiration related to impaired swallowing
- Planning: Patient will maintain airway safety during meals; patient will show gradual improvement in mobility; patient will participate in assisted movement; no signs of aspiration during feeding; blood pressure maintained within target range
- Implementation: Perform swallowing assessment before oral intake; keep patient NPO until cleared; position patient upright at 90 degrees during feeding; assist with passive and active range-of-motion exercises; monitor neurological status every 2–4 hours; administer antihypertensives as prescribed; collaborate with speech and physical therapy; ensure safety measures such as side rails and call light access
- Evaluation: Patient shows no signs of aspiration; swallowing improves with therapy; mobility increases with assistance; neurological status stabilizes; patient participates in care activities
Nursing Care Plan Example #8: Chronic Kidney Disease
Topic: Electrolyte Imbalance in Stage 4 CKD with Hyperkalemia Risk

- Assessment: Serum potassium 5.8 mEq/L; creatinine elevated; urine output decreased; blood pressure 156/94 mmHg; ECG shows peaked T waves; patient reports muscle weakness and fatigue; medical history includes advanced chronic kidney disease; dietary intake includes high-potassium foods
- Diagnosis: Risk for electrolyte imbalance related to impaired kidney function and decreased potassium excretion
- Planning: Serum potassium reduced to below 5.0 mEq/L within 24–48 hours; patient remains free of cardiac complications; patient identifies foods high in potassium to limit; vital signs remain stable
- Implementation: Monitor potassium levels and renal labs as ordered; place patient on cardiac monitoring; administer prescribed medications to reduce potassium (e.g., loop diuretics or potassium binders); restrict dietary potassium; monitor urine output every shift; assess for signs of worsening weakness or arrhythmias; notify healthcare providers immediately if potassium exceeds 6.0 mEq/L
- Evaluation: Potassium levels decrease toward the normal range; ECG changes resolve; patient reports reduced weakness; no cardiac complications observed; patient demonstrates understanding of dietary restrictions
Nursing Care Plan Example #9: COPD
Topic: COPD Exacerbation with Ineffective Airway Clearance

- Assessment: Respiratory rate 28/min; oxygen saturation 88% on room air; use of accessory muscles observed; productive cough with thick sputum; wheezing on auscultation; patient reports increased shortness of breath; history of chronic smoking; fatigue during minimal activity
- Diagnosis: Ineffective airway clearance related to increased mucus production and airway obstruction
- Planning: Oxygen saturation improves to above 92% with support; respiratory rate decreases below 22/min; patient demonstrates easier breathing; sputum becomes less thick and easier to clear
- Implementation: Administer oxygen at 1–2 L/min via nasal cannula as prescribed; monitor oxygen saturation every 2 hours; position patient in high-Fowler’s position; encourage controlled coughing and deep breathing exercises; administer bronchodilators and corticosteroids as ordered; ensure adequate hydration to thin secretions; monitor lung sounds each shift; notify healthcare providers if oxygen saturation remains below 90%
- Evaluation: Oxygen saturation stabilizes above 92%; respiratory effort decreases; wheezing reduces; sputum becomes thinner; patient reports improved breathing
If you're still unsure where to continue your studies, check out EssayService's article on the best colleges for nursing.
Nursing Care Plan Example #10: Major Depressive Disorder
Topic: Severe Depression with Risk for Self-Harm

- Assessment: Patient reports persistent low mood; expresses feelings of hopelessness; reduced appetite; sleep disturbance; limited eye contact; slow speech; history of previous depressive episodes; verbalizes passive thoughts about death; affect flat; minimal engagement during interaction
- Diagnosis: Risk for self-directed harm related to depressive symptoms and hopelessness
- Planning: Patient will verbalize at least one reason for safety within 24–48 hours; patient will engage in brief interactions with staff; patient will report reduced intensity of harmful thoughts; environment remains safe
- Implementation: Conduct safety checks at regular intervals; remove potentially harmful objects from the environment; maintain close observation based on risk level; encourage the patient to express thoughts freely; administer prescribed antidepressants; support a structured daily routine; involve mental health professionals; document mood changes and statements precisely
- Evaluation: Patient denies active self-harm intent; engagement with staff improves; mood shows slight stabilization; patient participates in care; no self-harm incidents observed
Too Many Patients Today?
Nursing school moves fast, and writing slows you down. Get help that keeps your assignments accurate and ready.
Wrapping Up
A nursing care plan starts with careful assessment, then moves step by step through the nursing process, where each part builds on the last. Once you collect the data, it leads you to a clear nursing diagnosis. That diagnosis determines your goals, which guide interventions, and those interventions are later evaluated as effective or ineffective. Hopefully, looking at the 10 samples in this article helped you understand how structured thinking will turn scattered patient information into organized care.
Frequently Asked Questions
How Do You Write a Nursing Care Plan Example?
How Do I Tell Which Nursing Diagnosis to Write First?
How Many Nursing Diagnoses are Included in One Plan?

John spends his days studying the impact of language. He uses his deep understanding of linguistics and research experience to help students communicate more effectively and craft immaculate research-intensive papers.
- How to Write a Nursing Care Plan - Harrier Grange Care Home. (2026). https://www.harriergrangecare.co.uk/. https://www.harriergrangecare.co.uk/news-events/how-to-write-a-nursing-care-plan/
- White, A. (2022, July 15). Nursing Care Plan | Learn the 5 Components of an Effective Care Plan. Nursing CE Central. https://nursingcecentral.com/nursing-care-plan/
- American Nurses Association. (2020). The Nursing Process. https://www.nursingworld.org/. https://www.nursingworld.org/practice-policy/workforce/what-is-nursing/the-nursing-process/


New posts to your inbox
Your submission has been received!